Intracranial pressure
Discuss the determinants of intracranial pressure
Definition and normal values
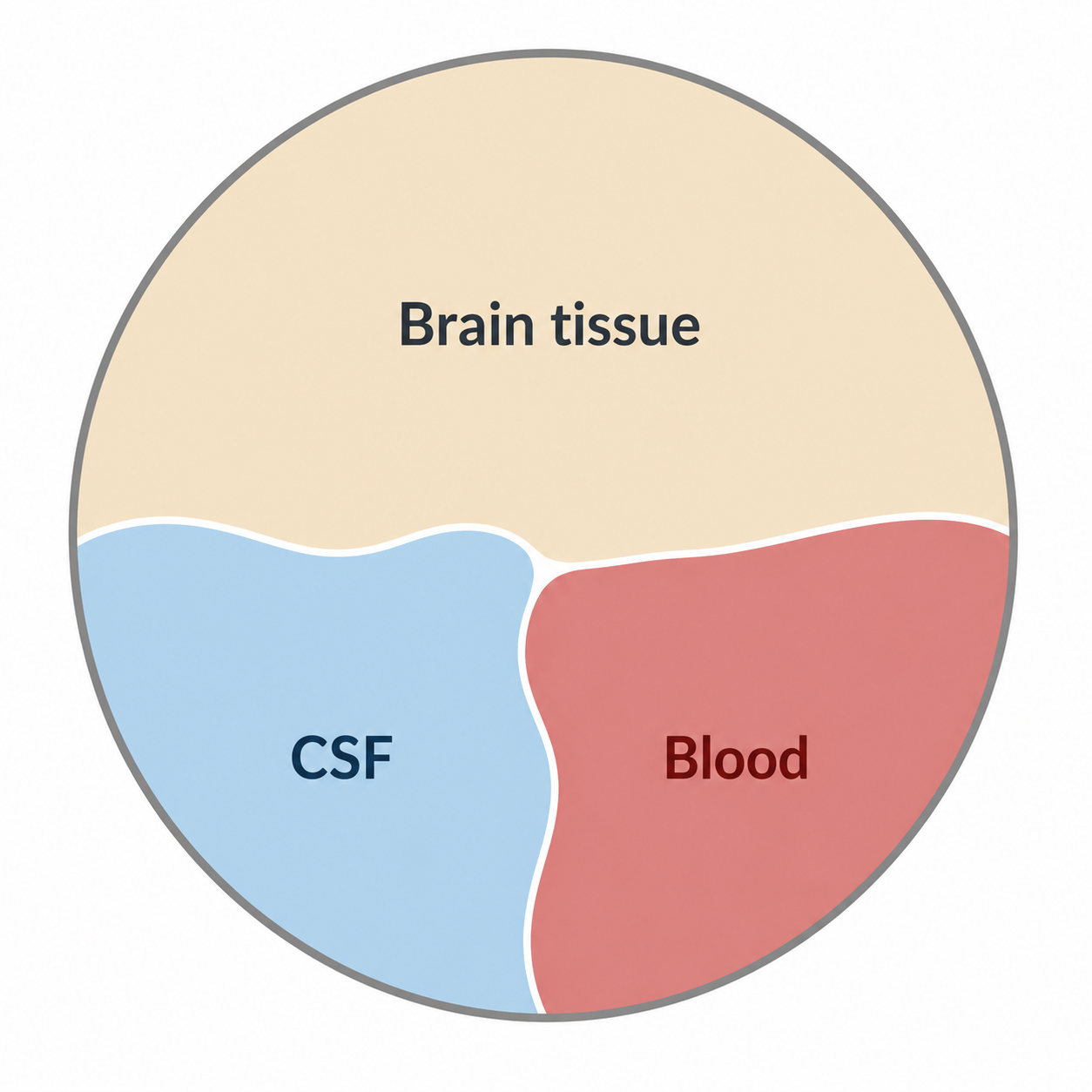
Intracranial pressure (ICP) is the pressure within the cranial vault, reflecting the combined volumes of brain tissue, blood, and cerebrospinal fluid (CSF).
In normal adults:
- ICP is 5–15 mmHg
- Sustained ICP >20 mmHg is associated with cerebral ischaemia
The cranial contents are distributed approximately as:
- Brain tissue: 1500 mL (~80%)
- Blood: 150 mL (~10%)
- CSF: 150 mL (~10%)
These proportions emphasise that ICP is determined by the interaction between compartments, not a single component.
Monroe–Kellie doctrine
The Monroe–Kellie doctrine describes the fundamental constraint governing ICP:
The cranium is a rigid, fixed-volume container. Therefore, an increase in one intracranial component must be offset by a decrease in another, otherwise ICP will rise.
This principle underpins all ICP physiology. Early in disease, compensatory mechanisms maintain ICP, but once exhausted, ICP rises rapidly.
Intracranial pressure-volume relationship and compensation
The relationship between intracranial volume and pressure is described by the intracranial pressure-volume curve.
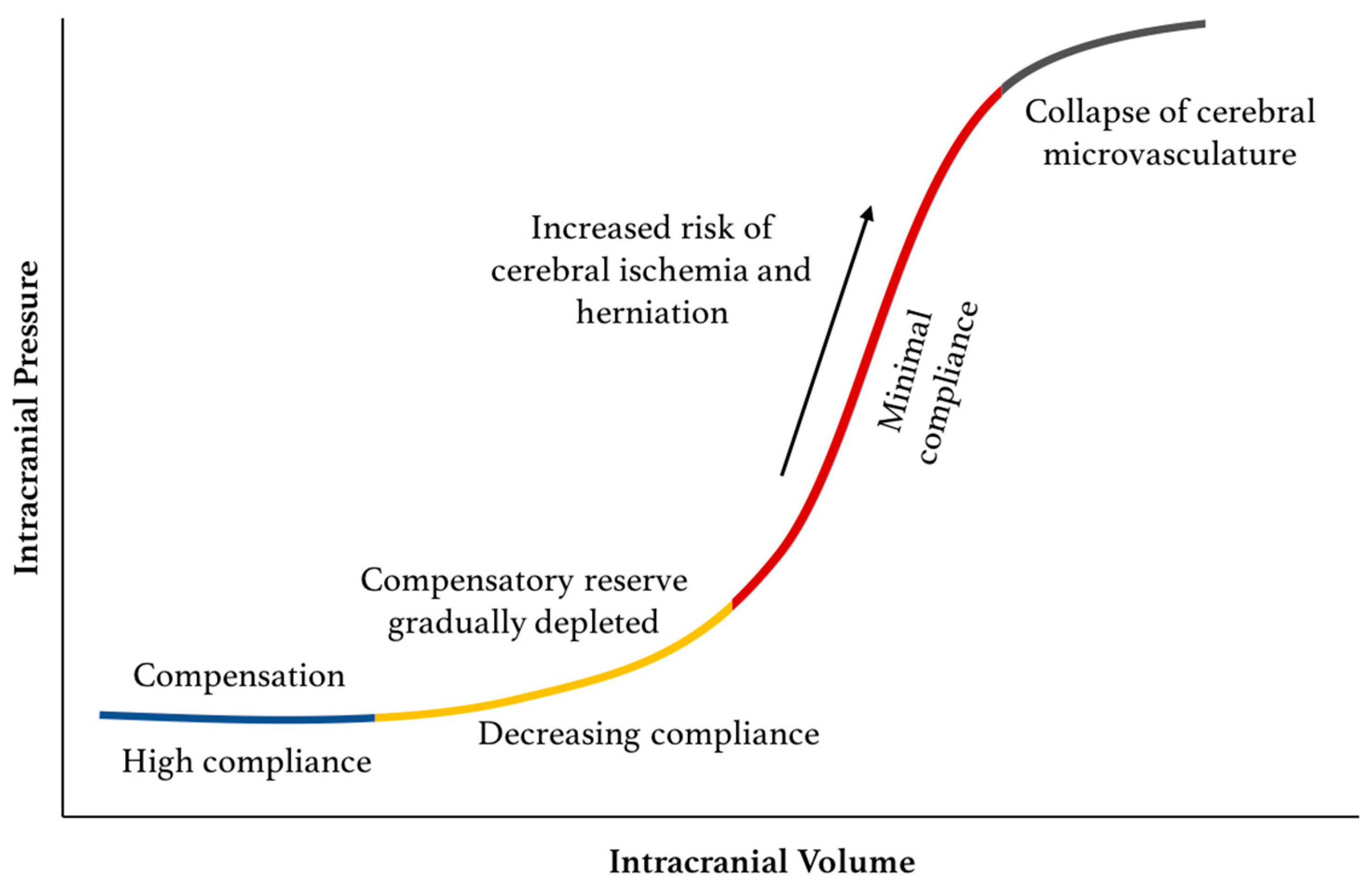
When ICP is low, changes in volume do not significantly affect ICP. However when ICP is higher, even small changes in volume can cause a massive rise in ICP.
By Harary et al. Intracranial Pressure Monitoring—Review and Avenues for Development.
Compensated phase
In the early phase, increases in volume produce minimal rises in ICP due to buffering:
- Venous blood displacement out of the cranial vault
- CSF displacement into the spinal subarachnoid space
- Increased CSF absorption via arachnoid granulations
CSF absorption is pressure dependent:
- Minimal when ICP <7 mmHg
- Rises linearly with ICP above this threshold
Decompensated phase
Once compensatory reserve is exhausted:
- Small increases in volume → large increases in ICP
- Leads to:
- ↓ CPP (CPP = MAP − ICP)
- ↓ CBF (CBF = CPP / vascular resistance)
- → cerebral ischaemia
Critical thresholds:
- ~20 mmHg → onset of ischaemia
- ~40 mmHg → critical ischaemia and risk of herniation
Cushing's reflex
Cushing's reflex is a late sign of severe intracranial hypertension.
Mechanism:
- ↑ ICP → ↓ CPP → brainstem ischaemia
- → massive sympathetic activation
Clinical features:
- Hypertension due to sympathetic activation
- Bradycardia mediated by the baroreceptor reflex response to hypertension
- Irregular respiration due to brainstem dysfunction or herniation
Determinants of intracranial pressure
Cranium
The cranium is normally fixed in volume.
A reduction in ICP occurs if cranial volume increases, for example due to decompressive craniectomy or open skull fracture.
Brain parenchyma
Brain parenchymal volume is generally not modifiable under normal physiological conditions. However, changes to brain tissue may occur due to pathological processes.
Increase in volume → ↑ICP:
- Tumour
- Abscess
- Intracranial haemorrhage
- Cerebral oedema
Decrease in volume → ↓ICP:
- Age-related atrophy
- Surgical resection
- Drainage of mass lesions
Cerebrospinal fluid (CSF)
CSF is produced by the choroid plexus (~500 mL/day) and absorbed via arachnoid granulations.
ICP depends on production and drainage:
-
↓ production → ↓ ICP (e.g. hypovolaemia)
-
↓ drainage → ↑ ICP (e.g. obstructive hydrocephalus)
-
↑ drainage → ↓ ICP (e.g. external ventricular drain (EVD) or ventriculoperitoneal shunt)